The Significance of Fibrosis Quantification as a Marker in Assessing Pseudo-Capsule Status and Clear Cell Renal Cell Carcinoma Prognosis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Tumor Sample Selection
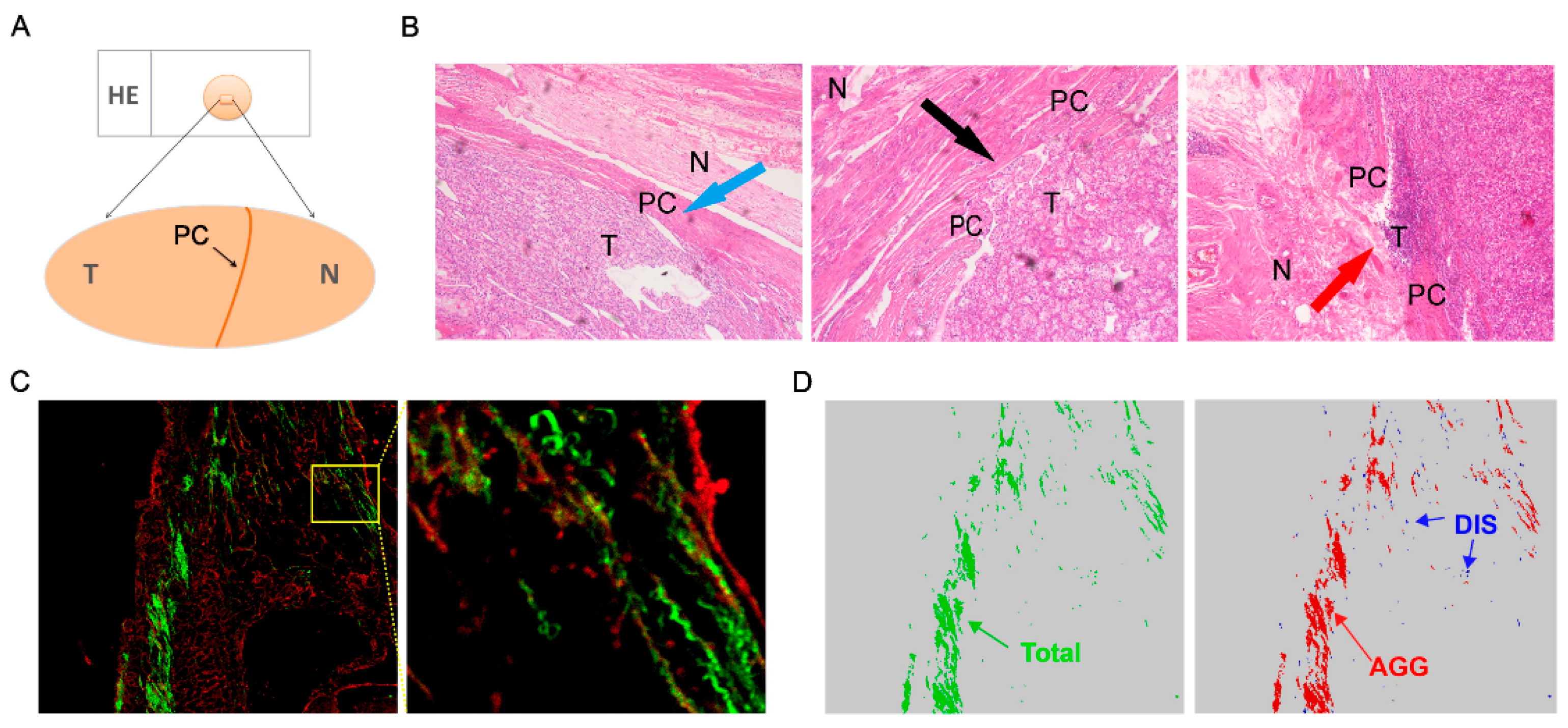
2.2. SHG and TPEF Imaging
2.3. Quantification of Collagen Morphology Parameters
2.4. Statistical Analysis
3. Results
3.1. Association between ITF and Clinicopathological Characteristics
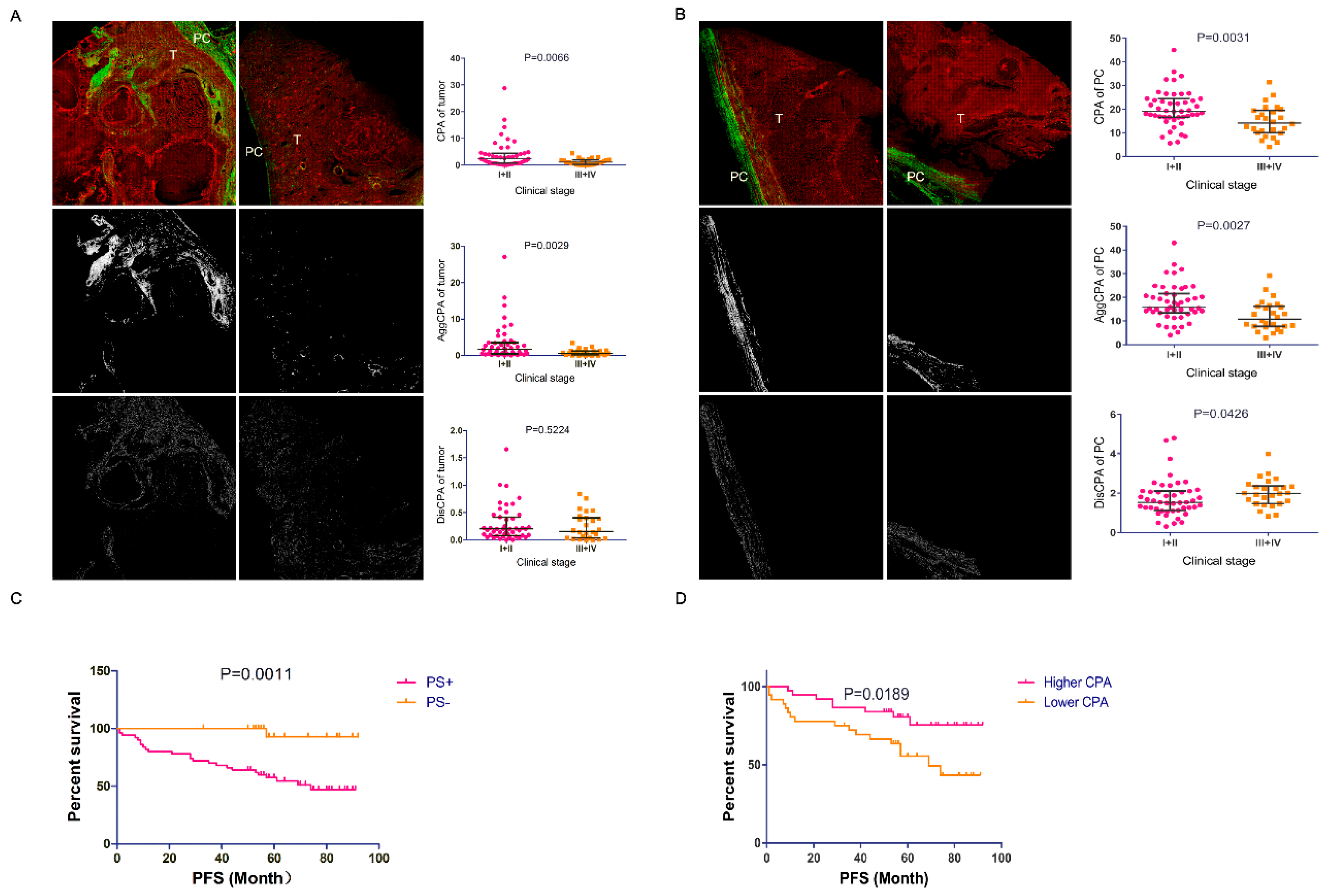
3.2. Association between PC Fibrosis and Clinicopathological Characteristics
3.3. PC fibrosis was a Marker for PC Invasion
3.4. The Prognostic Role of PC CPA as a Marker
4. Discussion
5. Conclusion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations:
| ccRCC | clear cell renal cell carcinoma |
| SHG/TPEF | second harmonic generation/two-photon excitation fluorescence |
| PC | Pseudo-capsule |
| CPA | collagen proportional area |
| AggCPA | percentage of aggregated collagen proportional area |
| DisCPA | percentage of distributed collagen proportional area |
References
- Takai, E.; Tsukimoto, M.; Kojima, S. TGF-β1 downregulates COX-2 expression leading to decrease of PGE2 production in human lung cancer A549 cells, which is involved in fibrotic response to TGF-β1. PLoS ONE 2013, 8, e76346. [Google Scholar] [CrossRef] [Green Version]
- Shabbir, M.; Gelister, J.S. Retroperitoneal fibrosis mimicking prostate cancer. J. R. Soc. Med. 2006, 99, 39–40. [Google Scholar] [CrossRef] [PubMed]
- Binkley, C.E.; Zhang, L.; Greenson, J.K.; Giordano, T.J.; Kuick, R.; Misek, D.; Hanash, S.; Logsdon, C.D.; Simeone, D.M. The molecular basis of pancreatic fibrosis: Common stromal gene expression in chronic pancreatitis and pancreatic adenocarcinoma. Pancreas 2004, 29, 254–263. [Google Scholar] [CrossRef]
- Mujtaba, S.S.; Ni, Y.B.; Tsang, J.Y.; Chan, S.K.; Yamaguchi, R.; Tanaka, M.; Tan, P.H.; Tse, G.M. Fibrotic focus in breast carcinomas: Relationship with prognostic parameters and biomarkers. Ann. Surg. Oncol. 2013, 20, 2842–2849. [Google Scholar] [CrossRef] [PubMed]
- Joung, J.W.; Oh, H.K.; Lee, S.J.; Kim, Y.A.; Jung, H.J. Significance of Intratumoral Fibrosis in Clear Cell Renal Cell Carcinoma. J. Pathol. Transl. Med. 2018, 52, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Xi, W.; Wang, J.; Liu, L.; Xiong, Y.; Qu, Y.; Lin, Z.; Chen, X.; Wang, Z.; Xu, J.; Guo, J. Evaluation of Tumor Pseudocapsule Status and its Prognostic Significance in Renal Cell Carcinoma. J. Urol. 2018, 199, 915–920. [Google Scholar] [CrossRef]
- Minervini, A.; Di Cristofano, C.; Lapini, A.; Marchi, M.; Lanzi, F.; Giubilei, G.; Tosi, N.; Tuccio, A.; Mancini, M.; Della Rocca, C.; et al. Histopathologic analysis of peritumoral pseudocapsule and surgical margin status after tumor enucleation for renal cell carcinoma. Eur. Urol. 2009, 55, 1410–1418. [Google Scholar] [CrossRef]
- Farris, A.B.; Adams, C.D.; Brousaides, N.; Della Pelle, P.A.; Collins, A.B.; Moradi, E.; Smith, R.N.; Grimm, P.C.; Colvin, R.B. Morphometric and visual evaluation of fibrosis in renal biopsies. J. Am. Soc. Nephrol. 2011, 22, 176–186. [Google Scholar] [CrossRef] [Green Version]
- Ranjit, S.; Dobrinskikh, E.; Montford, J.; Dvornikov, A.; Lehman, A.; Orlicky, D.J.; Nemenoff, R.; Gratton, E.; Levi, M.; Furgeson, S. Label-free fluorescence lifetime and second harmonic generation imaging microscopy improves quantification of experimental renal fibrosis. Kidney Int. 2016, 90, 1123–1128. [Google Scholar] [CrossRef] [Green Version]
- Capasso, A.; Viggiano, D.; Lee, M.W.; Palladino, G.; Bilancio, G.; Simeoni, M.; Capolongo, G.; Secondulfo, C.; Ronchi, A.; Caputo, A.; et al. Kidney Transplant Modifies the Architecture and Microenvironment of Basal Cell Carcinomas. Kidney Blood Press. Res. 2020, 45, 368–377. [Google Scholar] [CrossRef]
- Nigro, M.; Viggiano, D.; Ragone, V.; Trabace, T.; Di Palma, A.; Rossini, M.; Capasso, G.; Gesualdo, L.; Gigliotti, G. A cross-sectional study on the relationship between hematological data and quantitative morphological indices from kidney biopsies in different glomerular diseases. BMC Nephrol. 2018, 19, 62. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.W.; Liu, D.; Hu, J.M.; Xu, S.Y.; Zhuo, S.M.; Liu, Y.G.; Zhao, M. Application of Nonlinear Optical Microscopic Imaging Technology for Quality Assessment of Donor Kidneys. Transplant. Proc. 2018, 50, 3128–3134. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Hegde, S.; DeNardo, D.G. Tumor-associated fibrosis as a regulator of tumor immunity and response to immunotherapy. Cancer Immunol. Immunother. 2017, 66, 1037–1048. [Google Scholar] [CrossRef]
- Kato, T.; Noma, K.; Ohara, T.; Kashima, H.; Katsura, Y.; Sato, H.; Komoto, S.; Katsube, R.; Ninomiya, T.; Tazawa, H.; et al. Cancer-Associated Fibroblasts Affect Intratumoral CD8+ and FoxP3+ T Cells Via IL6 in the Tumor Microenvironment. Clin. Cancer Res. 2018, 24, 4820–4833. [Google Scholar] [CrossRef] [Green Version]
- Junttila, M.R.; De Sauvage, F.J. Influence of tumour micro-environment heterogeneity on therapeutic response. Nature 2013, 501, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Mezawa, Y.; Orimo, A. The roles of tumor- and metastasis-promoting carcinoma-associated fibroblasts in human carcinomas. Cell Tissue Res. 2016, 365, 675–689. [Google Scholar] [CrossRef]
- Klatte, T.; Chung, J.; Leppert, J.T.; Lam, J.S.; Pantuck, A.J.; Figlin, R.A.; Belldegrun, A.S. Prognostic relevance of capsular involvement and collecting system invasion in stage I and II renal cell carcinoma. BJU Int. 2007, 99, 821–824. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.J.; Kim, S.J.; Ha, U.S.; Hong, S.H.; Kim, J.C.; Choi, Y.J.; Hwang, T.K. Prognostic value of capsular invasion for localized clear-cell renal cell carcinoma. Eur. Urol. 2009, 56, 1006–1012. [Google Scholar] [CrossRef]
- May, M.; Brookman-Amissah, S.; Roigas, J.; Gilfrich, C.P.; Pflanz, S.; Hoschke, B.; Gunia, S. Evaluation of renicapsular involvement in Stages I and II renal cell carcinoma from the morphological and prognostic point of view. Urol. Oncol. 2010, 28, 274–279. [Google Scholar] [CrossRef]
- Papale, M.; Vocino, G.; Lucarelli, G.; Rutigliano, M.; Gigante, M.; Rocchetti, M.T.; Pesce, F.; Sanguedolce, F.; Bufo, P.; Battaglia, M.; et al. Urinary RKIP/p-RKIP is a potential diagnostic and prognostic marker of clear cell renal cell carcinoma. Oncotarget 2017, 8, 40412–40424. [Google Scholar] [CrossRef] [Green Version]
- Lucarelli, G.; Rutigliano, M.; Ferro, M.; Giglio, A.; Intini, A.; Triggiano, F.; Palazzo, S.; Gigante, M.; Castellano, G.; Ranieri, E.; et al. Activation of the kynurenine pathway predicts poor outcome in patients with clear cell renal cell carcinoma. Urol. Oncol. 2017, 35, e415–e427. [Google Scholar] [CrossRef] [PubMed]
- Lucarelli, G.; Rutigliano, M.; Sanguedolce, F.; Galleggiante, V.; Giglio, A.; Cagiano, S.; Bufo, P.; Maiorano, E.; Ribatti, D.; Ranieri, E.; et al. Increased Expression of the Autocrine Motility Factor is Associated With Poor Prognosis in Patients With Clear Cell-Renal Cell Carcinoma. Medicine 2015, 94, e2117. [Google Scholar] [CrossRef] [PubMed]
- Gigante, M.; Lucarelli, G.; Divella, C.; Netti, G.S.; Pontrelli, P.; Cafiero, C.; Grandaliano, G.; Castellano, G.; Rutigliano, M.; Stallone, G.; et al. Soluble Serum αKlotho Is a Potential Predictive Marker of Disease Progression in Clear Cell Renal Cell Carcinoma. Medicine 2015, 94, e1917. [Google Scholar] [CrossRef]
- Lucarelli, G.; Ditonno, P.; Bettocchi, C.; Vavallo, A.; Rutigliano, M.; Galleggiante, V.; Larocca, A.M.; Castellano, G.; Gesualdo, L.; Grandaliano, G.; et al. Diagnostic and prognostic role of preoperative circulating CA 15-3, CA 125, and beta-2 microglobulin in renal cell carcinoma. Dis. Markers 2014, 2014, 689795. [Google Scholar] [CrossRef]
- Lucarelli, G.; Loizzo, D.; Franzin, R.; Battaglia, S.; Ferro, M.; Cantiello, F.; Castellano, G.; Bettocchi, C.; Ditonno, P.; Battaglia, M. Metabolomic insights into pathophysiological mechanisms and biomarker discovery in clear cell renal cell carcinoma. Expert. Rev. Mol. Diagn. 2019, 19, 397–407. [Google Scholar] [CrossRef]
- Bianchi, C.; Meregalli, C.; Bombelli, S.; Di Stefano, V.; Salerno, F.; Torsello, B.; De Marco, S.; Bovo, G.; Cifola, I.; Mangano, E.; et al. The glucose and lipid metabolism reprogramming is grade-dependent in clear cell renal cell carcinoma primary cultures and is targetable to modulate cell viability and proliferation. Oncotarget 2017, 8, 113502–113515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucarelli, G.; Rutigliano, M.; Sallustio, F.; Ribatti, D.; Giglio, A.; Lepore Signorile, M.; Grossi, V.; Sanese, P.; Napoli, A.; Maiorano, E.; et al. Integrated multi-omics characterization reveals a distinctive metabolic signature and the role of NDUFA4L2 in promoting angiogenesis, chemoresistance, and mitochondrial dysfunction in clear cell renal cell carcinoma. Aging 2018, 10, 3957–3985. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, T.P.; Stuart, M.; Oosting, J.; Tollenaar, R.; Sier, C.F.M.; Mesker, W.E. Increased expression of cancer-associated fibroblast markers at the invasive front and its association with tumor-stroma ratio in colorectal cancer. BMC Cancer 2019, 19, 284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, F.T.; Sun, W.; Zhang, J.T.; Fan, Y.Z. Cancer-associated fibroblast regulation of tumor neo-angiogenesis as a therapeutic target in cancer. Oncol. Lett. 2019, 17, 3055–3065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Outschoorn, U.E.; Pavlides, S.; Whitaker-Menezes, D.; Daumer, K.M.; Milliman, J.N.; Chiavarina, B.; Migneco, G.; Witkiewicz, A.K.; Martinez-Cantarin, M.P.; Flomenberg, N.; et al. Tumor cells induce the cancer associated fibroblast phenotype via caveolin-1 degradation: Implications for breast cancer and DCIS therapy with autophagy inhibitors. Cell Cycle 2010, 9, 2423–2433. [Google Scholar] [CrossRef] [Green Version]
- Willis, B.C.; Borok, Z. TGF-beta-induced EMT: Mechanisms and implications for fibrotic lung disease. Am. J. Physiol. Lung Cell. Mol. Physiol. 2007, 293, L525–L534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, W.; Jackson, K.; McGuire, P.G. Degradation of type IV collagen by matrix metalloproteinases is an important step in the epithelial-mesenchymal transformation of the endocardial cushions. Dev. Biol. 2000, 227, 606–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harb, O.A.; Elfeky, M.A.; El Shafaay, B.S.; Taha, H.F.; Osman, G.; Harera, I.S.; Gertallah, L.M.; Abdelmonem, D.M.; Embaby, A. SPOP, ZEB-1 and E-cadherin expression in clear cell renal cell carcinoma (cc-RCC): Clinicopathological and prognostic significance. Pathophysiology 2018, 25, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Liu, X.; Cheng, Q.; Zhu, S.; Bai, J.; Zheng, J. RUNX3 regulates renal cell carcinoma metastasis via targeting miR-6780a-5p/E-cadherin/EMT signaling axis. Oncotarget 2017, 8, 101042–101056. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Features | Number, n (n = 73) | |
|---|---|---|
| Gender | Male | 54 |
| Female | 19 | |
| Age(years) | ≤58 | 39 |
| >58 | 34 | |
| Fuhrman grade | G1+2 | 54 |
| G3+4 | 19 | |
| Clinical stage | I+II | 47 |
| III+IV | 26 | |
| Tumor size | ≤4 cm | 47 |
| >4 cm | 26 | |
| Intra-tumoral necrosis | Absent | 54 |
| Present | 19 | |
| PC status | PS- | 23 |
| PS+ | 50 |
| Factors | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| OR(95% CI) | p Value | OR(95% CI) | p Value | ||
| Gender | male vs. female | 0.995 (0.323–3.066) | 0.994 | ||
| Age (year) | ≤58 vs. >58 | 1.200 (0.444–3.241) | 0.719 | ||
| Nuclear Grade | G1+2 vs. G3+4 | 1.400 (0.436–4.499) | 0.572 | 1.019 (0.274–3.782) | 0.978 |
| Clinical Stage | I + II vsIII + IV | 3.732 (1.108–12.569) | 0.034 | 2.128 (0.563–8.043) | 0.265 |
| Tumor Size | ≤4 cm vs. >4 cm | 5.679 (1.495–21.577) | 0.011 | 6.409 (1.453–28.264) | 0.014 |
| Intra-tumoral necrosis | absent vs. present | 1.400 (0.436–4.499) | 0.572 | ||
| Tumor side | left vs. right | 0.562 (0.206–1.537) | 0.261 | ||
| PC | CPA | 0.925 (0.863–0.992) | 0.028 | 0.923 (0.854–0.998) | 0.044 |
| AggCPA | 0.925 (0.864–0.991) | 0.026 | |||
| DisCPA | 1.116 (0.620–2.008) | 0.714 | |||
| Tumor | CPA | 0.942 (0.845–1.051) | 0.285 | ||
| AggCPA | 0.942 (0.840–1.057) | 0.312 | |||
| DisCPA | 0.399 (0.078–2.026) | 0.268 | |||
| Factors | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | ||
| Gender | male vs. female | 0.493 (0.169–1.435) | 0.194 | ||
| Age (year) | ≤58 vs. >58 | 0.943 (0.428–2.078) | 0.884 | ||
| Fuhrman Grade | G1+2 vs. G2+4 | 1.532 (0.660–3.588) | 0.321 | 1.259 (0.526–3.013) | 0.605 |
| Clinical Stage | I+II vs III + IV | 2.036 (0.926–4.475) | 0.077 | 0.823 (0.324–2.093) | 0.682 |
| Tumor Size | ≤4 cm vs. >4 cm | 2.562 (1.159–5.662) | 0.020 | 1.462 (0.608–3.512) | 0.396 |
| Tumor side | left vs. right | 0.634 (0.273–1.470) | 0.288 | ||
| Histologic Necrosis | Absent vs. present | 2.781 (1.259–6.142) | 0.011 | 2.858 (1.084–7.533) | 0.034 |
| PS status | PS- vs. PS+ | 12.957 (1.751–95.869) | 0.012 | 10.529 (1.362–81.419) | 0.024 |
| CPA | 0.938 (0.883–0.996) | 0.037 | 0.949 (0.889–1.013) | 0.116 | |
| PS | AggCPA | 0.928 (0.870–0.991) | 0.025 | ||
| DisCPA | 1.449 (0.948–2.213) | 0.087 | |||
| CPA | 1.025 (0.939–1.120) | 0.577 | |||
| Tumor | AggCPA | 1.027 (0.935–1.127) | 0.578 | ||
| DisCPA | 1.470 (0.411–5.258) | 0.554 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qin, C.; Yin, H.; Liu, H.; Liu, F.; Du, Y.; Xu, T. The Significance of Fibrosis Quantification as a Marker in Assessing Pseudo-Capsule Status and Clear Cell Renal Cell Carcinoma Prognosis. Diagnostics 2020, 10, 895. https://doi.org/10.3390/diagnostics10110895
Qin C, Yin H, Liu H, Liu F, Du Y, Xu T. The Significance of Fibrosis Quantification as a Marker in Assessing Pseudo-Capsule Status and Clear Cell Renal Cell Carcinoma Prognosis. Diagnostics. 2020; 10(11):895. https://doi.org/10.3390/diagnostics10110895
Chicago/Turabian StyleQin, Caipeng, Huaqi Yin, Huixin Liu, Feng Liu, Yiqing Du, and Tao Xu. 2020. "The Significance of Fibrosis Quantification as a Marker in Assessing Pseudo-Capsule Status and Clear Cell Renal Cell Carcinoma Prognosis" Diagnostics 10, no. 11: 895. https://doi.org/10.3390/diagnostics10110895