1. Introduction
Hepatocellular carcinoma (HCC) is the fourth most common cause of cancer deaths around the world [
1]. It is also the fifth most commonly diagnosed cancer and is the second most common cause of cancer deaths in Taiwan [
2]. The majority of HCC (75–80%) cases are attributable to persistent viral infections with the hepatitis B virus (HBV) (50–65%) and hepatitis C virus (HCV) (10–15%) in Taiwan [
3]. Carcinogenesis of HCC is a very complex multi-factor process, including viral or non-viral causes such as alcoholic hepatitis and nonalcoholic steatohepatitis (NASH) [
4]. Chronic hepatitis infection causes liver inflammation and damage, subsequent fibrosis, and liver regeneration that may lead to malignant transformation of the liver [
5]. In early-stage HCC, potentially curative treatments are available. They include surgical resection, percutaneous ablation, and liver transplantation. Percutaneous ablation and liver transplantation can only be applied in carefully selected patients depending on the patient’s tumor status and general condition as well donor availability. Therefore, surgical resection is the most commonly used curative management of HCC. However, the recurrence rate is high after resection, especially within the first two years [
6]. About 50% to 90% of postoperative deaths after curative resection are a result of recurrence of the disease, and intrahepatic recurrence accounts for the majority of cases. Liver fibrosis has been thought to increase the risk of intrahepatic recurrence after hepatectomy in the case of HCC [
7].
Conventional histological staging of fibrosis, such as the Ishak fibrotic score, is highly subjective and prone to sampling error and observer variations. Second harmonic generation and two-photon microscopy was first used as a comprehensive, morphology-based, quantified method for scoring liver fibrosis [
8,
9,
10]. qFibrosis uses a system of second harmonic generation plus two-photon excitation fluorescence (SHG/TPEF) microscopy to image tissue samples and establish an index by (i) identification of different collagen patterns, (ii) extraction of collagen architectural features, and (iii) statistical analysis of features of the respective collagen patterns. qFibrosis scoring has been analyzed employing Metavir and Ishak fibrosis staging as standard references and has been established as a fully-quantitative, innovative method incorporating histological features to facilitate accurate fibrosis scoring in animal models and chronic hepatitis B patients [
11]. Besides this, it was also applied to quantitatively identify subtle changes of liver fibrosis in chronic hepatitis B patients following antiviral therapy as well as to accurately assess fibrosis in non-alcoholic fatty liver disease patients in more recent studies [
12,
13,
14]. Therefore, this study involves the use of this more accurate fibrosis scoring method to evaluate the fibrotic status of the hepatic tissue of patients with HCC after hepatectomy.
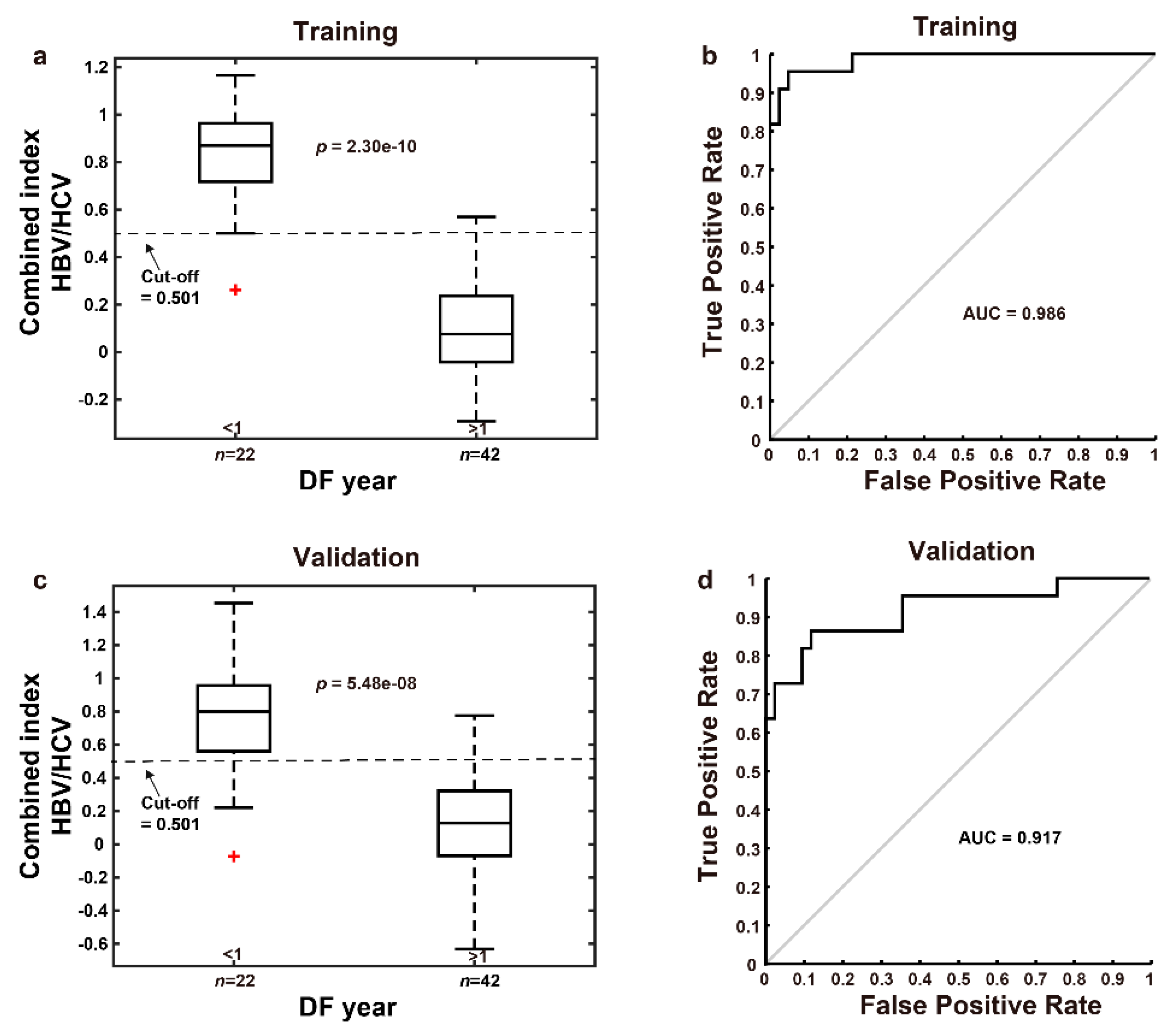
The application of qFibrosis is intended enable the prediction of early recurrence after curative intent hepatectomy according to the fibrotic features of hepatic tissue. Thus, patients identified as high-risk for early recurrence can be followed more carefully in shorter intervals following hepatectomy. In this study, we generated a “combined index” using multi-dimensional artificial intelligence analysis of qFibrosis with the features of fibrosis from 81 patients receiving partial hepatectomy. When the combined index is larger than 0.501, early recurrence is more likely.
2. Materials and Methods
2.1. Study Population
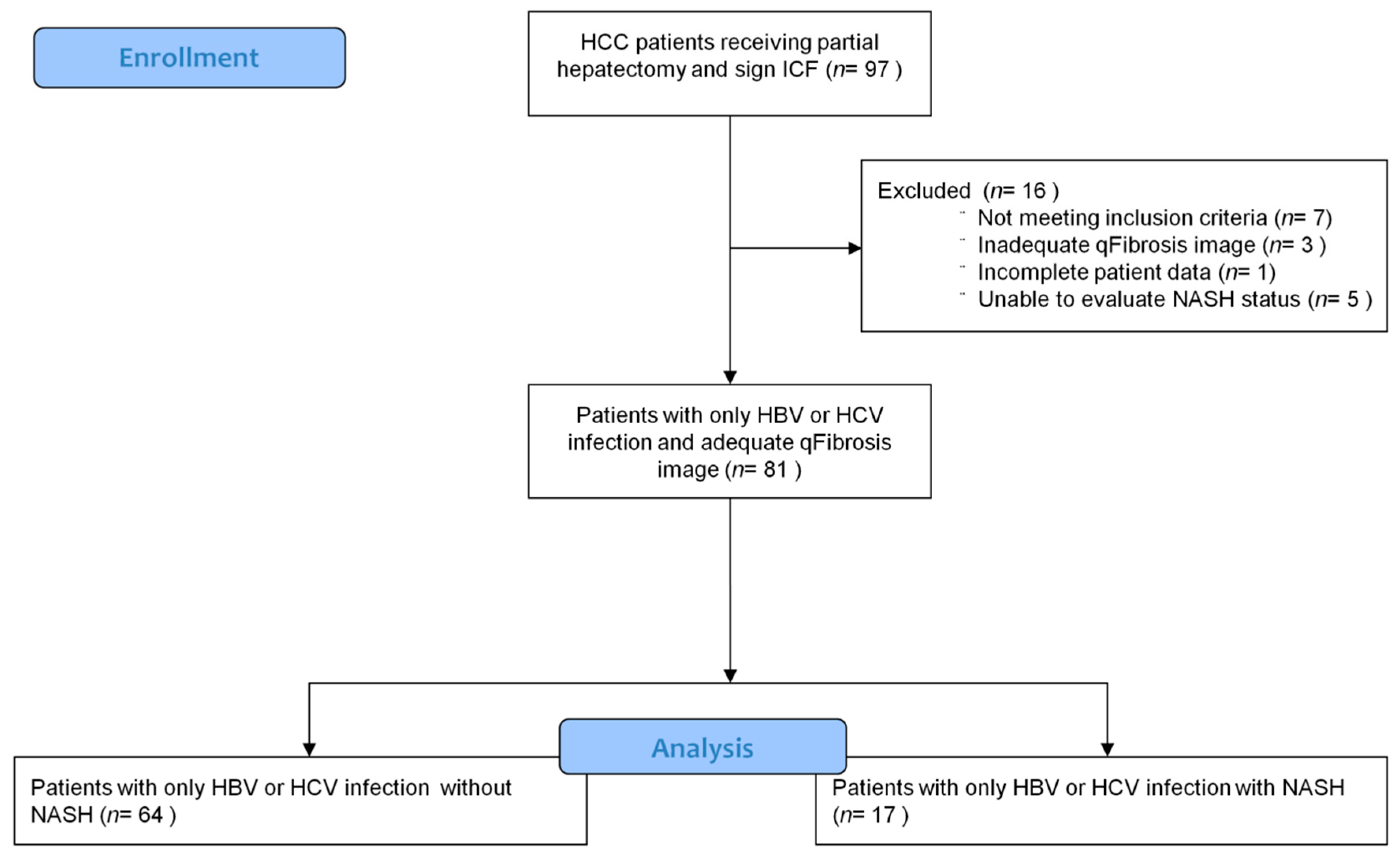
Adult patients who were diagnosed and staged by liver tumor biopsy, abdomen triphasic computed tomography (CT), and alpha fetoprotein (AFP) as resectable HCC with known HBV or HCV infection and planning to have curative intent surgical resection were enrolled in this study. Patients with co-infection of HBV and HCV, inadequate tissue samples or history of other malignancy within 2 years prior to screening were excluded (detailed inclusion and exclusion criteria as
Table S1). These patients receive regular follow-up with abdomen triphasic CT after surgery. Informed consent regarding use of tissue samples, clinical data, and medical records for this research was obtained from all enrolled patients. The clinical and pathological staging used in this study was The American Joint Committee on Cancer (AJCC) 7th edition. All experimental protocols and study methods conformed to the ethical guidelines of the Declaration of Helsinki and were approved by the Institutional Review Board of Human Research at National Cheng Kung University Hospital and Chi Mei Medical Center.
2.2. Image Acquisition System
Images were acquired on unstained sections of non-tumor liver samples, using a Genesis (HistoIndex Pte. Ltd, Singapore) system, in which second harmonic generation (SHG) microscopy was used to visualize collagen, and the other cell structures were visualized using two-photon excited fluorescence (TPEF) microscopy.
The samples were laser-excited at 780 nm; SHG signals were recorded at 390 nm, and TPEF signals were recorded at 550 nm. Image acquisition was performed at a 20× magnification for each 200 × 200 μm2 image. Multiple adjacent images were captured to encompass large areas. To cover most of the sample areas, 10 five-by-five multi-tile images were acquired for each human sample, with a final image size of 10 mm2 (10 × 1 × 1 mm).
2.3. Image Quantification
Total collagen percentages and other collagen features, including specific collagen strings and collagen connectivity-related measurements, were used to predict early recurrence (disease free (DF) < 1 year) and late recurrence (DF ≥ 1 years) post operation HCC.
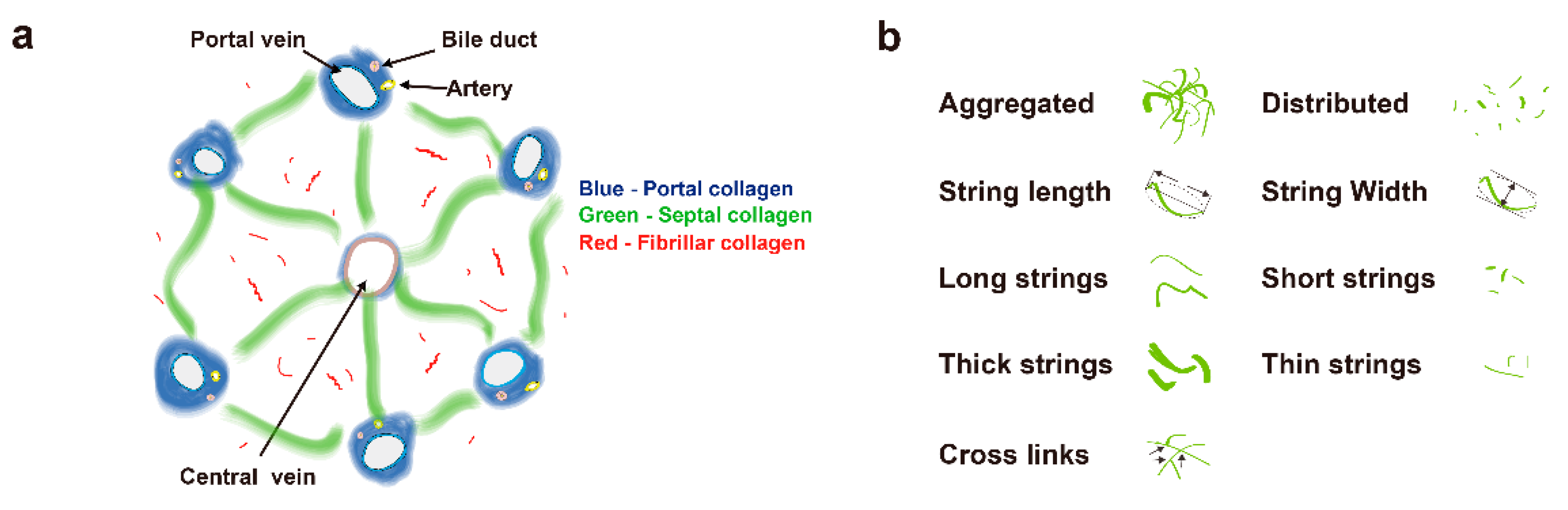
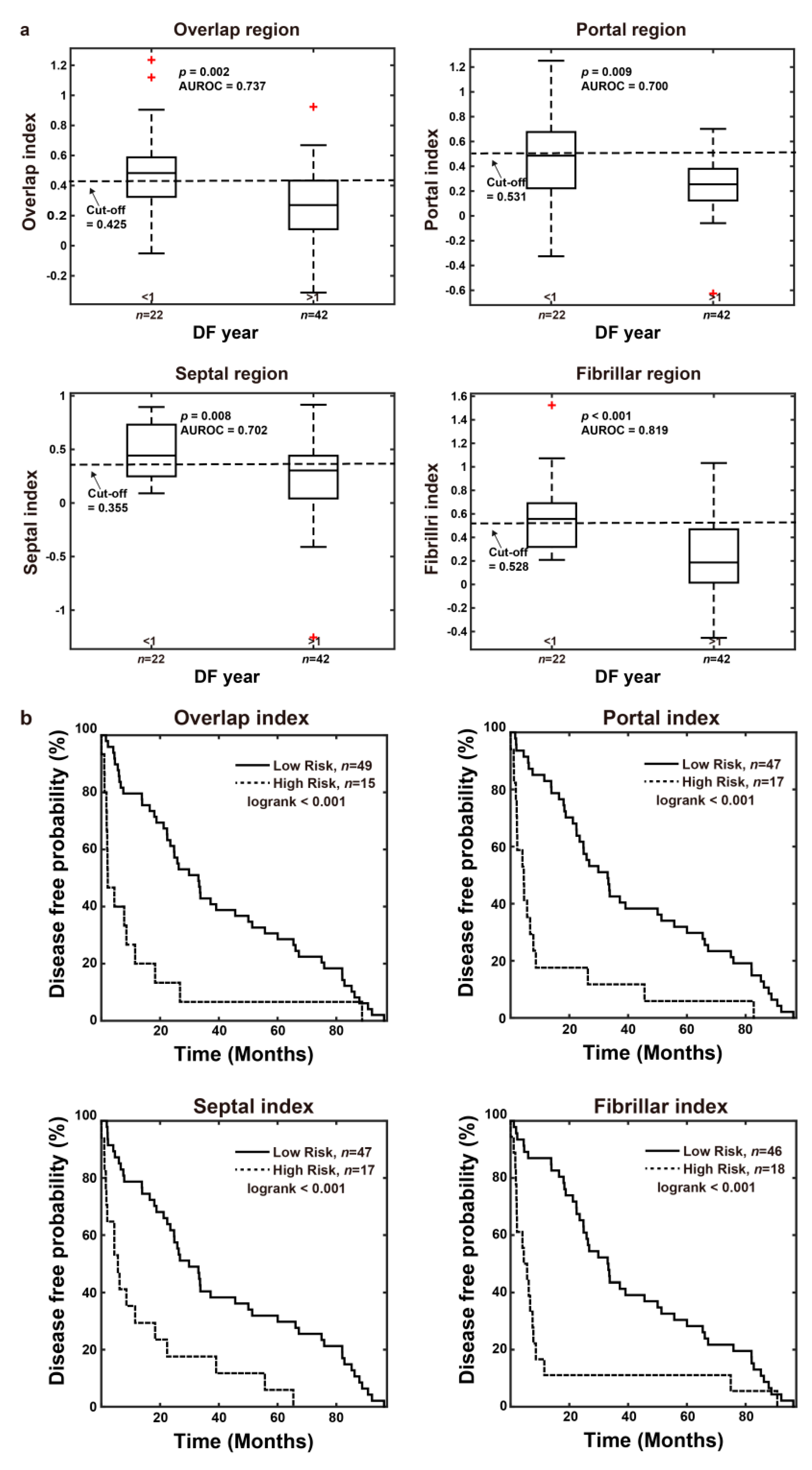
A total of 100 morphological features were initially used in this study. Collagen in the overall region was classified into three specific areas: portal collagen (portal expansion), septal collagen (bridging fibrosis), and fibrillar collagen (fine collagen distributed in the pericellular/perisinusoidal space) [
11]. Furthermore, in addition to the total measures, collagen was also measured in two different patterns, namely, distributed collagen (fine collagen) and aggregated collagen (large patches). For each pattern in these specific regions (portal, septal, and fibrillar), collagen strings were categorized into short strings, long strings, thin strings, and thick strings according to string length and width (
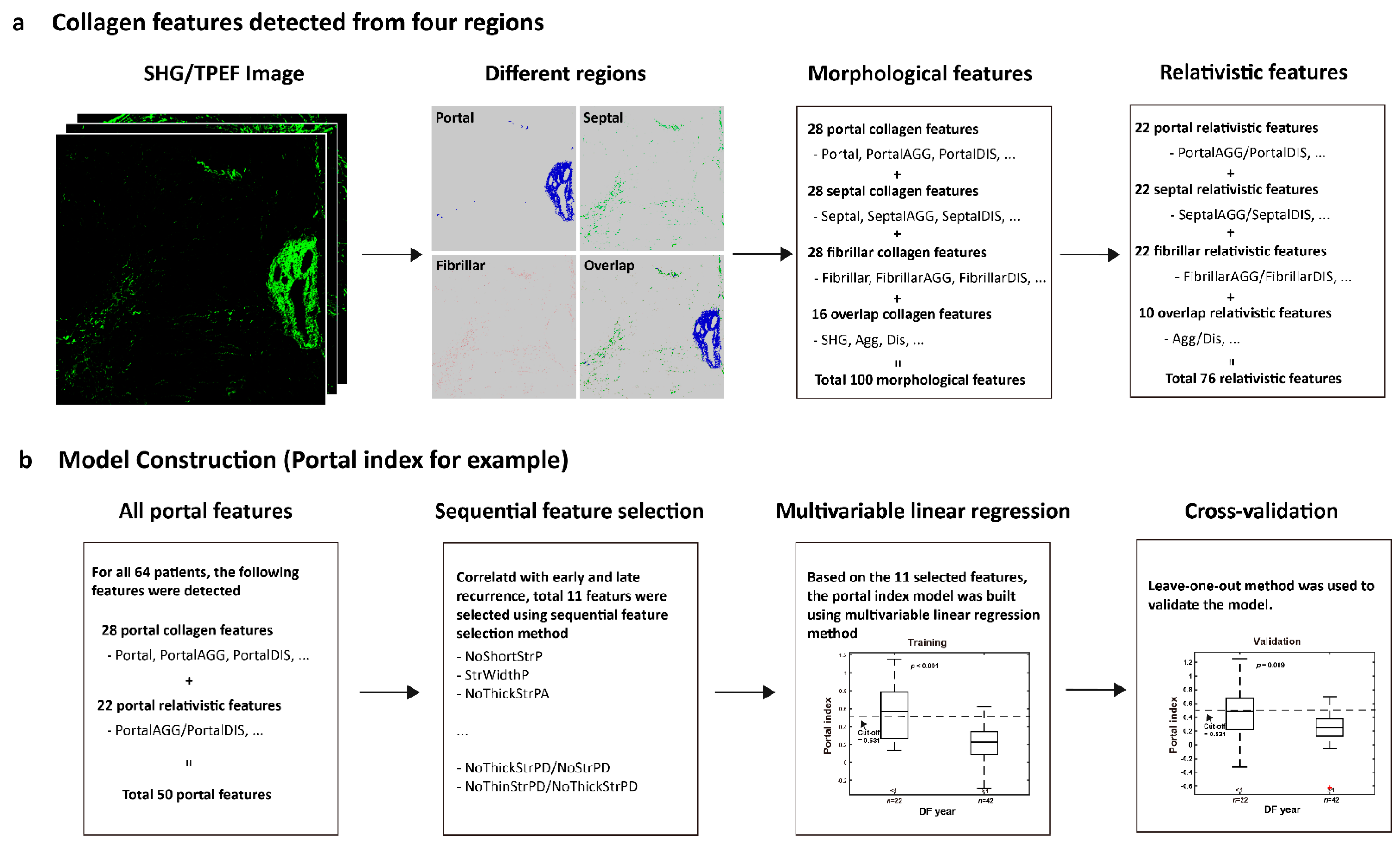
Figure 1a,b). Based on the 100 collagen morphological features, another 76 relativistic features were constructed. Each relativistic feature was the ratio of two morphological features, such as the ratio of the number of short strings to the number of long strings (NoShortStr/NoLongStr) and the ratio of aggregated collagen to distributed collagen (AGG/DIS). Thus, total 176 features were used for model construction (
Figure 2a).
2.4. Model Construction
To predict early recurrence in patients with hepatocellular carcinoma after curative hepatectomy, a prediction model was developed based on the quantified collagen features.
Firstly, each feature was normalized to a value between 0–1 according to its maximum and minimum values. Secondly, feature selection was performed to reduce the dimensionality of data by selecting only a subset of collagen features. A common method of feature selection, named sequential feature selection was used in this study [
15]. In the procedure of sequential feature selection, a linear regression model was used whereby the criterion was the residual sum of squares and the search algorithm was sequential forward selection. In total, 64 cases with HBV or HCV but no NASH were used to find the most significant collagen features related with early recurrence.
Next, a model was trained to predict early recurrence in patients with hepatocellular carcinoma after curative hepatectomy using a “combined index”, which was constructed from the previously mentioned 64 cases with multivariable linear regression method. To validate the prediction model, leave-one-out cross-validation method was used [
16,
17]. Briefly, one sample is randomly retained as the validation data while the remaining 63 cases are used as training data to construct the model. The performance of the prediction model is then tested on the single validation case. The cross-validation process is repeated 64 times, with a different case left out each time. The data of combined index for statistical analysis in the study, in the absence of special note was the prediction values by leave-one-out cross-validation method.
Thus, for each HCC patient after hepatectomy, a combined index can be calculated on the SHG/TPEF image using the recurrence prediction model (
Figure 2b). This feature indicates that a higher value of the combined index correlates with early recurrence.
2.5. Statistical Analysis
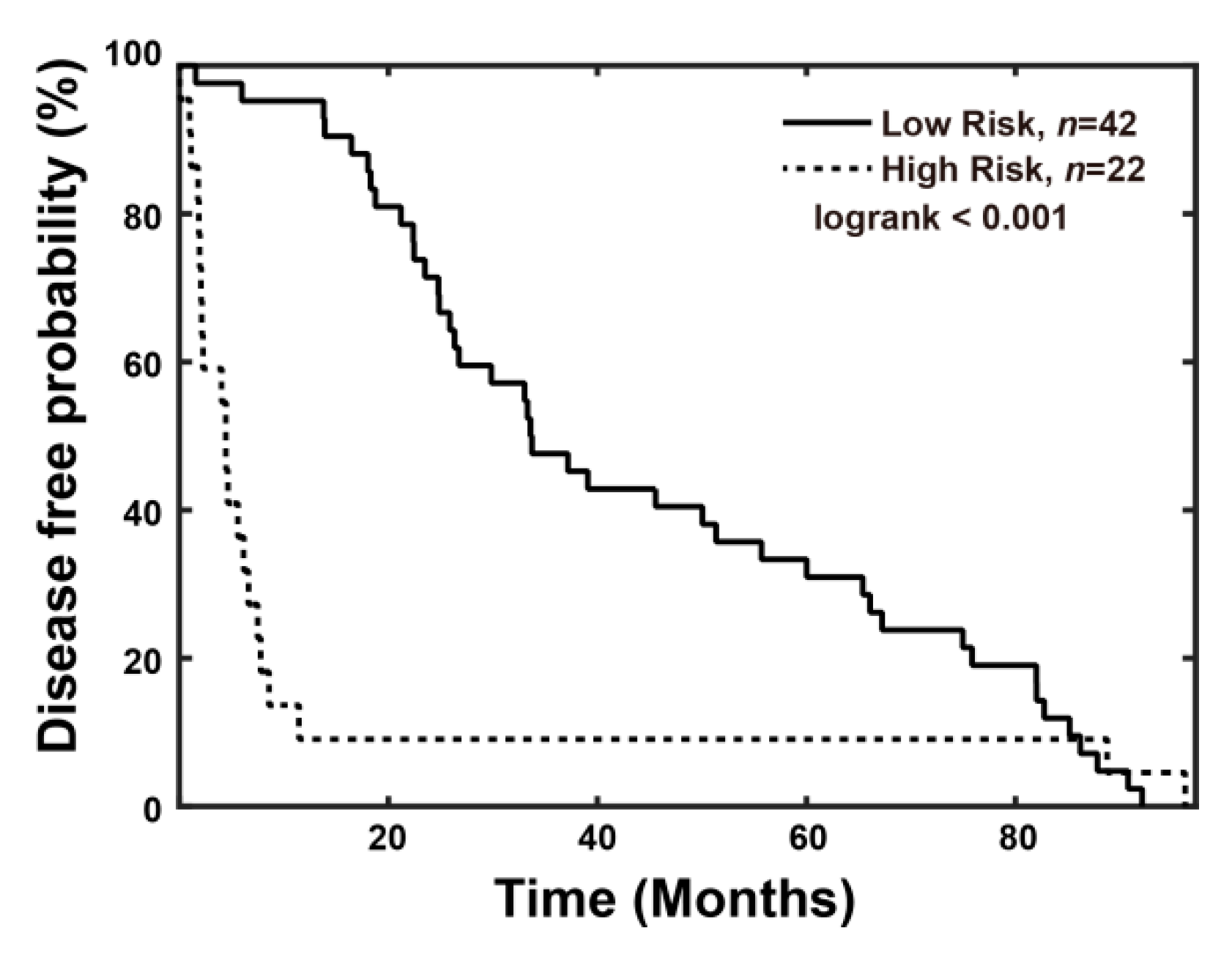
The two-tailed Wilcoxon rank-sum test was performed to estimate the statistical differences of combined index between early and late recurrence. To assess the predictive effect, a receiver operating characteristic curve analysis was used to estimate the area under the curve. Disease-free curves were calculated using the Kaplan–Meier method, and distributions were compared using the log-rank test. Disease-specific overall survival was calculated from the date of diagnosis until disease-caused death or the end of follow-up. A univariate COX regression analysis was used to assess the association between each variable and survival/recurrence. A Cox proportional hazards model was used in the multivariate analyses and was also used to estimate Hazard Ratios (HRs) and their 95% confidence intervals (CIs).
4. Discussion
Currently, HCC is still one of the leading causes of cancer deaths worldwide. Partial hepatectomy remains the most commonly used method to cure patients. However, high recurrence rates have been observed after curative intent hepatectomy. According to previous studies, liver fibrosis increases the risk of intrahepatic recurrence after hepatectomy or radiofrequency ablation for HCC [
7,
20]. Traditional histological fibrotic staging systems, such as the Ishak fibrotic score, although the current standard, are criticized for their subjective interpretation due to either sampling error or observer variations. qFibrosis provides a fully-quantitative method incorporating histological features to obtain more accurate fibrosis scoring for the liver. Our study results indicated that the combined index calculated using qFibrosis may predict early recurrence of HCC after curative intent hepatectomy.
qFibrosis has shown its ability to perform accurate fibrotic scoring of hepatic tissue in animal models and chronic hepatitis B patients. Besides, it had been established as a better way for screening and enrollment of NASH patients in clinical trials [
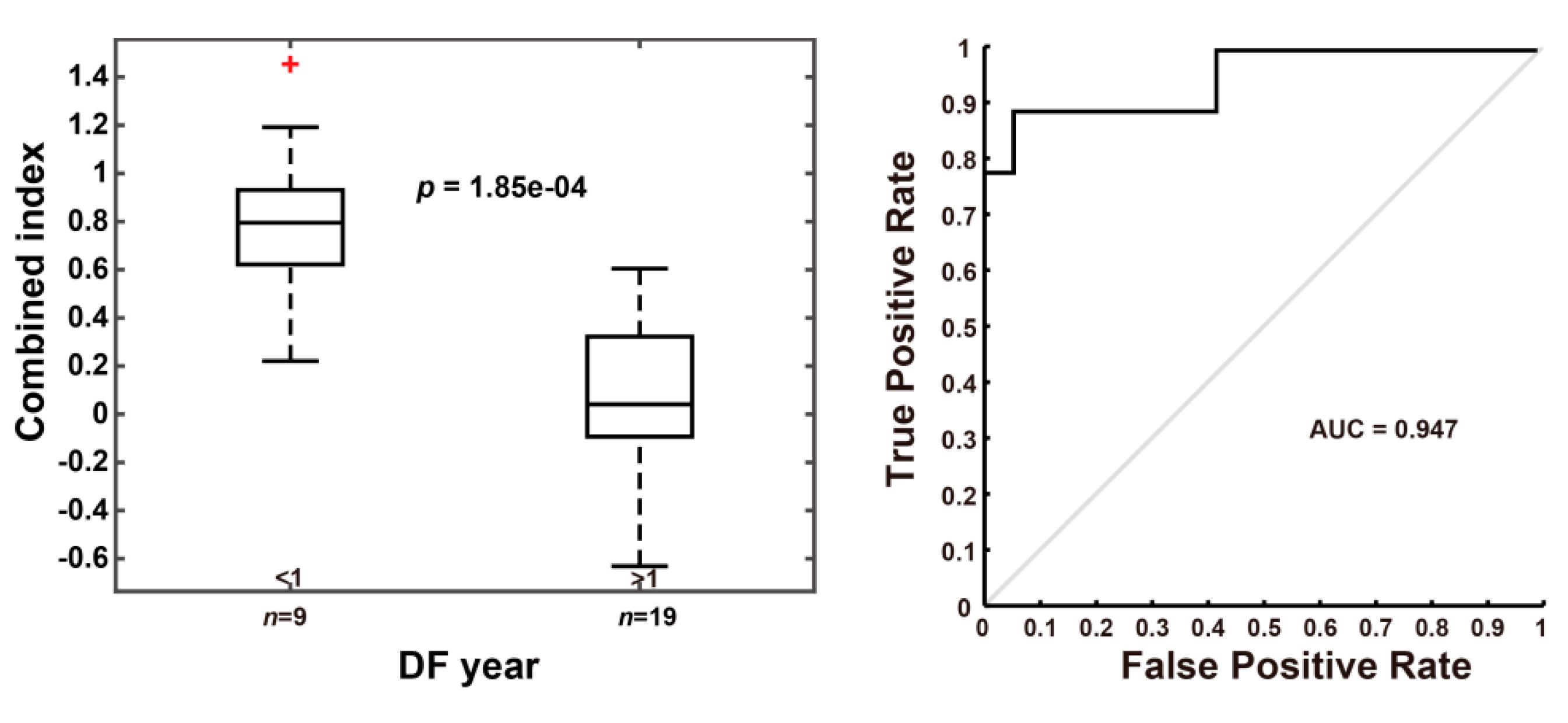
21,
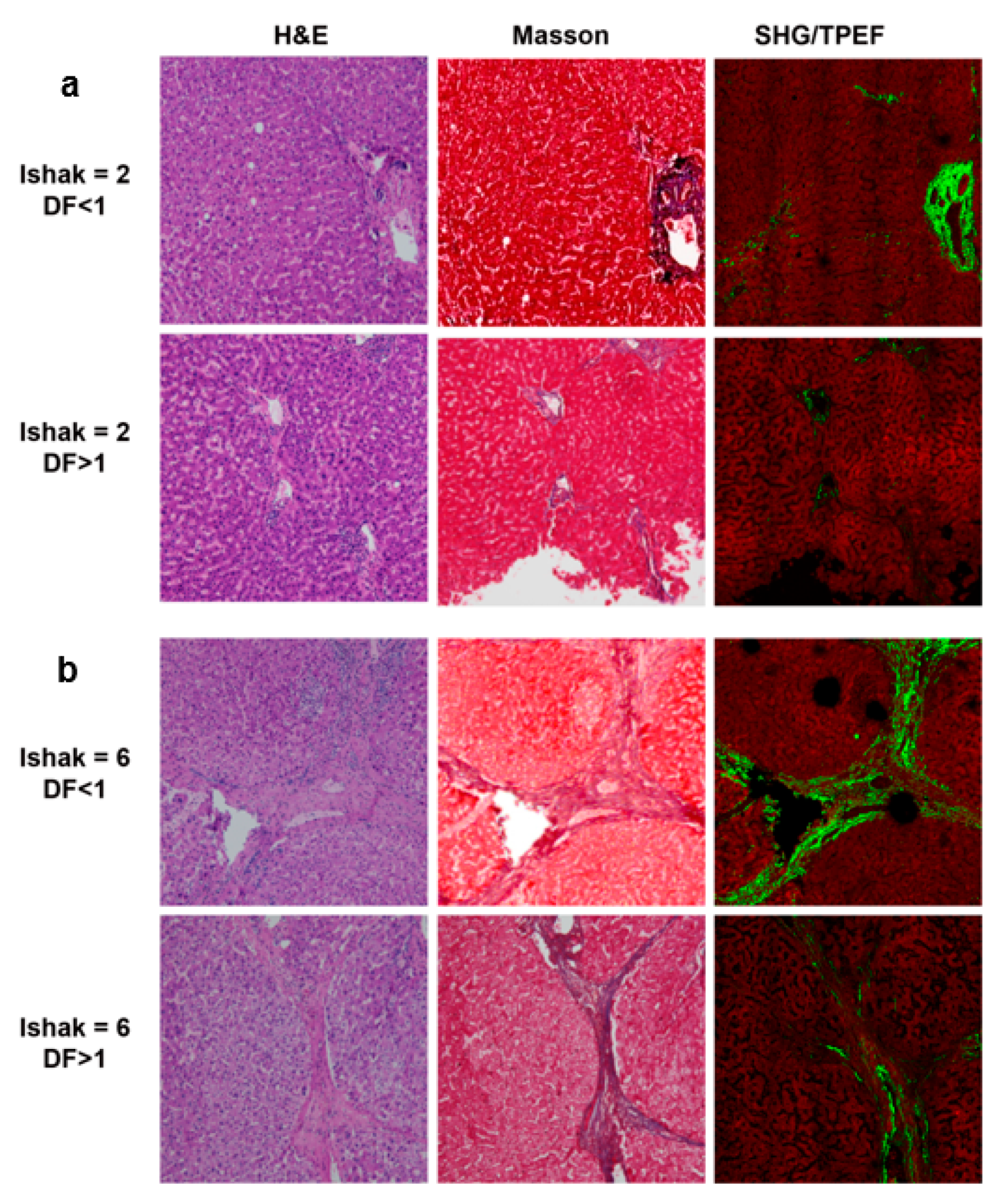
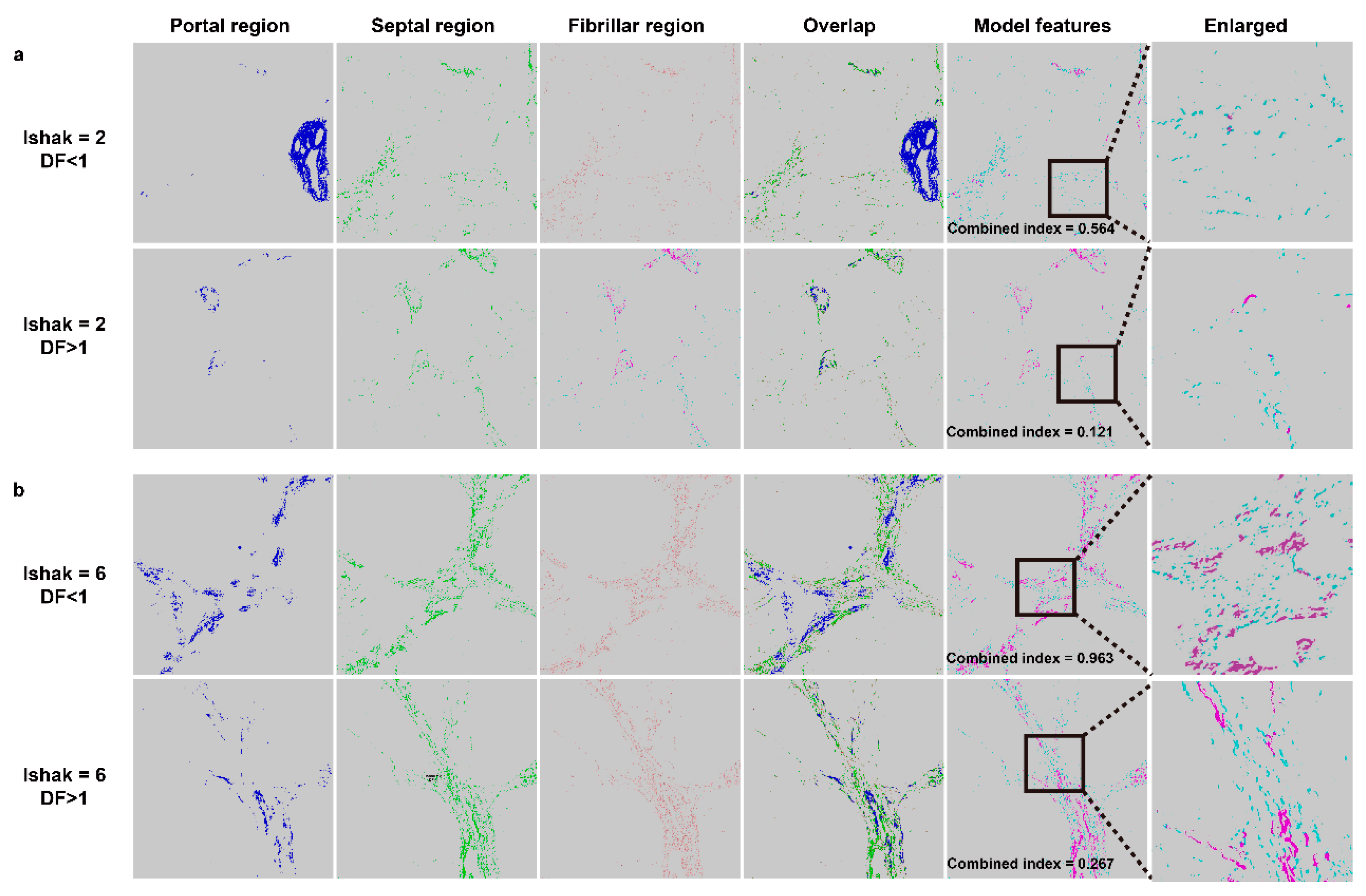
22]. Our results using the recurrence prediction model in 64 HCC patients after hepatectomy indicated that early recurrence can be predicted when the combined index is more than 0.501. Ko et al. reported that histological evidence of fibrosis of the underlying liver tissue is the most significant predictive factor of intrahepatic recurrence. Our novel method can be used to determine differences in fibrotic status when the samples are scored the same by the Ishak system, as shown in
Figure 4a,b. Therefore, using this method will make it possible to follow high-risk patients more carefully and also consider other treatment according to the risks of disease recurrence.
It is known that there are also many non-invasive tools for evaluation of fibrotic status [
23,
24,
25,
26,
27]. Many of them use serum markers, which may be influenced largely by the inflammation status of the patient. In addition, some of these markers may not be specific for the liver. Some image-based non-invasive methods arrive at indeterminate results for fibrotic status in up to 33% of cases, which is not satisfactory by today’s medical standards [
28]. Artificial intelligence has been widely applied in modern precision medicine for several years, with some applications focusing on digital pathology images [
29], others on interpretation of multiple data or radiological images [
30,
31,
32,
33]. In our study, we simply used qFibrosis to obtain the accurate fibrotic status of the resected liver sample, and processed the specific features with the clinical data using multi-dimensional artificial intelligence analysis. As the result, the “combined index” showed good prediction ability in early recurrence of HCC.
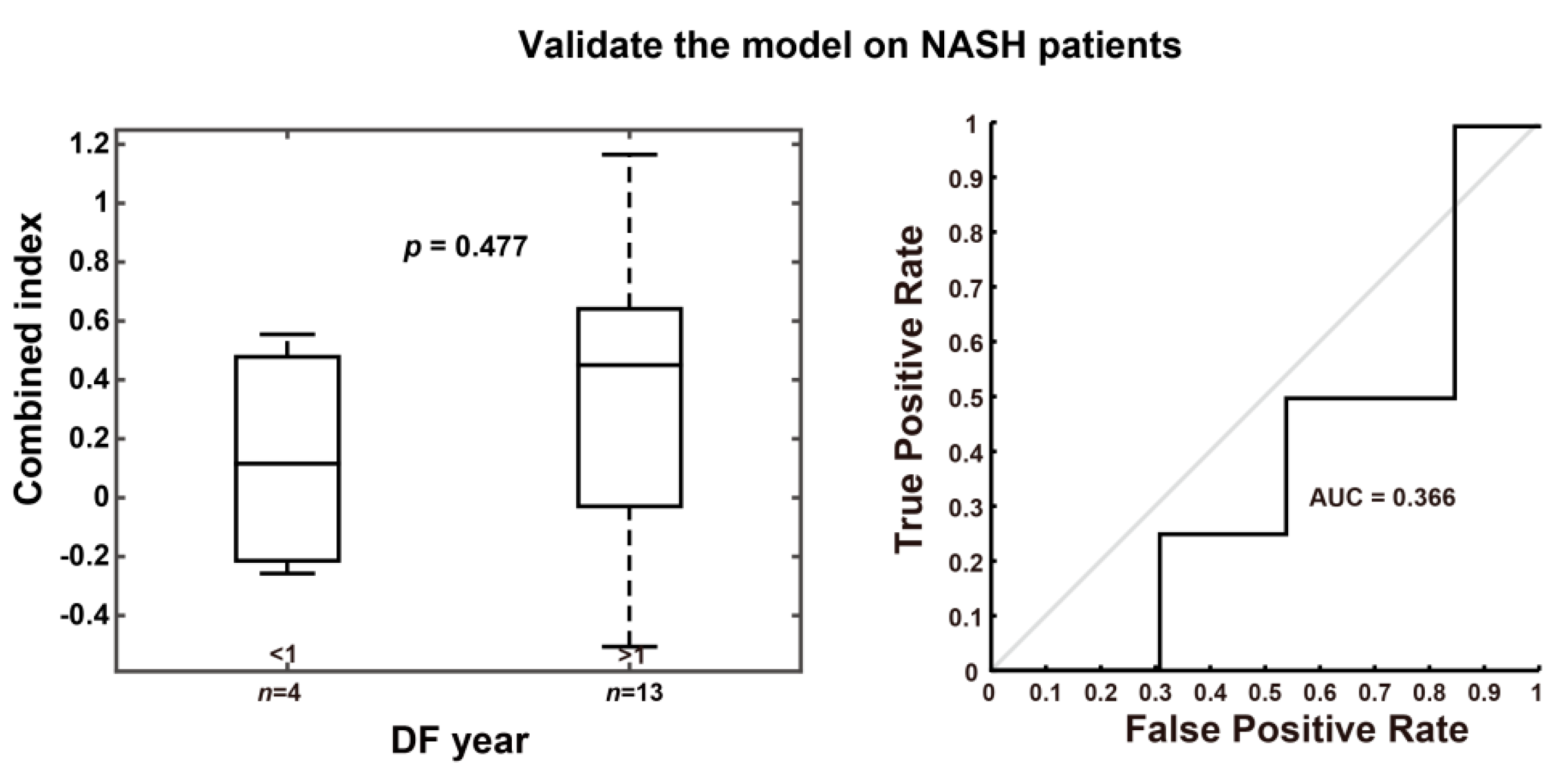
Viral and non-viral related HCC are thought to have different pathologic mechanisms in progression of normal liver tissue to liver cancer. We had applied the combined index, which derived from the viral related non-NASH HCC patients, in other HCC patients with NASH features, and it was unable to predict early recurrence in these NASH patients. Therefore, the fibrotic pattern of liver tissue may be different in the viral and non-viral related HCC patients, and further study is needed.
There were some limitations to this study. First, it was hard for us to collect another group of patients for external validation, so we used a leave-one-out cross-validation method to overcome this problem. Second, although qFibrosis can provide more accurate fibrotic status than conventional histological methods, sampling error may still have some influence on the qFibrosis score. Besides, our study was unable to provide competing risk analysis as Metroticket 2.0 model used in liver transplantation patients owing to the complicated clinical situations and the study design [
34,
35]. Finally, our method needs liver tissue to obtain its qFibrosis score, so it is not a non-invasive assessment of liver fibrosis.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}









